AbstractAny intelligent fool can make things bigger, more complex, and more violent. It takes a touch of genius – and a lot of courage to move in the opposite direction.
E. F. Schumacher (1911–1977)
Economist and author
In Small Is Beautiful (1973)
Frugal innovations have the potential to offer simple and cost-effective solutions to the healthcare challenges of the world. However, despite the potential for frugal innovations in healthcare, this context has been rarely studied. The objective of this article is to shed some light on patterns of frugal innovations in healthcare and thereby contribute to the literature. With this aim, we conducted a comprehensive literature review and searched for innovations that were labelled as frugal and were related to healthcare. This led us to a sample of 50 frugal innovations in the healthcare sector. For each of the 50 selected examples, we examined various characteristics of the innovation, such as the country of origin, first launch market, type of innovator, type of innovation, type of care, and geographic diffusion. Our findings show that most of the frugal innovations originated in the United States, followed by India. The most frequent first launch market was India. In terms of types of innovators, academia seemed to be the strongest driver. Most frugal innovations are product innovations in the fields of neonatology and general practice. In this article, we expand on these findings and examine the relationships between individual variables to reveal further insights. Finally, we offer conclusions, an outlook for frugal innovation in the healthcare sector, and future research questions.
Introduction
The philosophy behind the development of frugal innovation has been described as “instead of adding more bells and whistles, they strip their products down to their bare essentials” (The Economist, 2010). Various researchers have since tried to define frugal innovation and differentiate the term from similar terms such as low-cost innovation, good-enough innovation, jugaad innovation, frugal engineering, constraint-based innovation, Gandhian innovation, or reverse innovation (e.g., Bhatti and Ventresca, 2013; Brem & Wolfram, 2014; Ostraszewska & Tylec, 2015; Zeschky et al., 2014). Weyrauch and Herstatt (2016) have analyzed various definitions and recommend that an innovation should be considered as frugal if it meets the following relevant criteria: a substantial reduction of cost, the concentration on core functionalities, and optimized performance levels.
Frugal innovations have been adopted in a wide range of industries including automotive, energy, information and communication technology, and healthcare. One of the most prominent products is certainly the TATA Nano, introduced in 2009 as the world’s cheapest family car created for the needs of Indian and Chinese families at a remarkable cost of only $2000 USD (Prahalad, 2012). Other examples of frugal innovation in other sectors include the Mitticool refrigerator, a natural refrigerator made entirely from clay, and GE Healthcare’s high-efficiency Lullaby baby warmer for neonatal care. In each case, the frugal innovations in these examples were developed for the needs of emerging economies.
Researchers in the field of frugal innovation have predominantly explored the differences and similarities of frugal innovation with respect to other types of innovation (Brem & Wolfram, 2014; Landrum, 2007; Weyrauch & Herstatt, 2016; Zeschky et al., 2014). Others have conducted case studies that discuss the relationship between frugal innovation and sustainability (Kahle et al., 2013; Pansera & Sarkar, 2016; Rosca et al., 2016; Tiwari et al., 2016) or the importance of frugal innovation for the competitiveness of multinational corporations (Agarwal & Brem, 2012; Anderson & Markides, 2007; Tiwari & Herstatt, 2012). Only a limited number of studies have focused on the potential of frugal innovation to improve global health and primarily conduct case studies on singular frugal innovations (e.g., Ramdorai & Herstatt, 2015).
Access to healthcare and wellbeing is a human right. Despite the progress that has been made worldwide in recent years to improve healthcare access and wellbeing, inequalities in healthcare still continue to exist (UN, 2015). For example, fifty percent of women in developing regions do not have access to adequate healthcare services; every year six million children die before reaching the age of five, and epidemics such as HIV/AIDS “thrive where fear and discrimination limit people’s ability to receive the services they need to live healthy and productive lives” (UN, 2015). So, despite some global progress, health is still a major issue worldwide. Indeed, the United Nations has proclaimed that “ensuring healthy lives and promoting the wellbeing for all at all ages is essential to sustainable development” and has made this issue the third of its “17 goals to transform our world” (UN, 2015).
In our view, frugal innovations have the potential to contribute to the achievement of this goal. Thus, the aim of this article is to shed more light on possible patterns of frugal innovation in healthcare by taking a closer look at 50 examples of frugal innovation in this sector. The article is structured as follows. In the next section, we provide the theoretical background. We then describe the methodology and findings of our empirical study. Finally, we close with a conclusion on the outlook for frugal innovation in healthcare, discuss potential limitations of our study, and provide recommendations for further research.
Theoretical Background
Frugal innovations have the potential to contribute to achieving sustainable development goals. Several studies highlighting the link between frugal innovation and sustainability often outline prominent healthcare examples such as Aravind Eye Care Systems or Narayana Hrudayalaya (e.g., Allen et al., 2016; Basu et al., 2013; Hossain, 2016; Kahle et al., 2013; Oppong, 2015; Rosca et al., 2016; Sarangi et al., 2014; Tiwari & Herstatt, 2012). Kahle and colleagues (2013) provide support for the notion that the creation of more inclusive markets through frugal innovation contributes to socioeconomic development, which in turn strengthens democratization and state building. The authors also point out that multinational corporations can have a positive impact on democratization by offering for-profit products and services to serve bottom-of-the-pyramid (BOP) markets.
The bottom of the pyramid is an untapped market of more than four billion people worldwide living their lives on less than two US dollars per day (Prahalad, 2004). The management thinker Prahalad and his colleagues initiated the BOP market approach more than two decades after E.F. Schumacher’s movement of “appropriate technologies” as a development approach based on technology to address socioeconomic challenges in developing countries (Schumacher, 1973). They argued for market-based solutions for poverty by including billions of people in the formal economy (Prahalad & Lieberthal, 1998). Addressing these markets would require “radical innovations in technology and business models” (Prahalad & Hart, 2002; Ramdorai & Herstatt, 2015; Prahalad & Lieberthal, 1998). They presented several frugal low-cost innovations from emerging markets that provide essential functionality and fit to the local needs (Prahalad, 2004; Prahalad & Hammond, 2002). This exposure to the concept created immense interest in academia and industry.
Despite the importance of frugal innovations in improving global health, the literature on frugal innovation in healthcare is rather scarce and consists mostly of case studies (Hossain, 2016). As mentioned above, prominent cases of frugal innovation in healthcare are the Aravind Eye Care System (Clyde, 2005) and Narayana Hrudayalaya (Khanna et al., 2005). The Aravind Eye Care System is a network of ophthalmology hospitals that treats most of its patients for free or at a subsidized rate and still is economically viable due to its ability to decrease cost dramatically through innovation. A similar example – also from India – is Narayana Hrudayalaya, which provides quality cardiological services to the poor. While both approaches have a process and product innovation at their core, there are also multiple examples of product innovations from multinational corporations. GE Healthcare has been very active in developing healthcare products for the BOP market, including the Lullaby and Embrace low-cost infant warmers or the MAC electrocardiogram series priced at only a fraction of the products sold in industrialized countries (Ramdorai & Herstatt, 2015).
With this study, we try to shed more light on patterns of frugal innovations in healthcare by studying a variety of frugal innovations with respect to their innovation characteristics. This effort brings out the features of these innovations and further highlights the potential of frugal innovation to improve global health.
Empirical Analysis
To identify examples of frugal innovation in healthcare, a comprehensive literature review using five databases (Cochrane, EBSCO, Google Scholar, Scopus, and Web of Science) and following the PRISMA approach was conducted between August 2016 and March 2017 (PRISMA, 2018). We used the two search strings “frugal innovations in healthcare” and “frugal innovation AND healthcare.” The English search terms bear a risk of creating, first, a bias towards frugal innovations from industrialized countries and, second, a bias towards frugal innovations from multinational corporations and academia compared to grassroots entrepreneurs from emerging or developing countries. Despite these limitations, our study should still shed light on the current scarcity of literature on frugal innovations in healthcare. We only included cases that fulfill the criteria of frugality as defined in the introduction above. If sufficient information about an innovation and its frugality could not be found, it was discarded. In total, 45 examples were discarded based on the above-mentioned criteria and 50 frugal innovations were selected for the study. For these 50 innovations, we retrieved information on different innovation characteristics. We explored the country of origin, first launch market, type of innovator, type of innovation, medical specialty, WHO healthcare and essential health services coverage categories, and geographic diffusion measured as the number of countries the innovation is distributed to. Information on each variable was gathered through an Internet search for the innovation or on the innovator’s website, publications, or news articles describing the innovation. We then analyzed the variables across the 50 cases as well as the relationships between variables using contingency tables. Due to the small sample size, we report descriptive results only.
Entrepreneur’s country of origin and first launch market
The country of origin is usually associated with the country where a product is produced or made. In order to differentiate the country of origin – specifically with respect to multinational companies – we differentiate between the entrepreneur’s country of origin and the first launch market. The entrepreneur’s country of origin is thus defined as the country where the entrepreneur is from or was originally founded (e.g., in the case of GE the United States). We also segment the results into continents and according to the International Monetary Fund’s classification into either advanced or emerging and developing economies (IMF, 2017).
For 21 out of 50 frugal healthcare innovations, the entrepreneur’s country of origin was the United States, whereas India and the Netherlands represented 7 and 5 out of 50 innovations (Figure 1). Looking at continents, exactly half of the frugal innovations’ entrepreneurs were from North America, followed by Europe with 12 out of 50 innovations. Three quarters of frugal healthcare innovation entrepreneurs in our sample (38 out of 50) thus have their origin in the industrialized countries of the world.
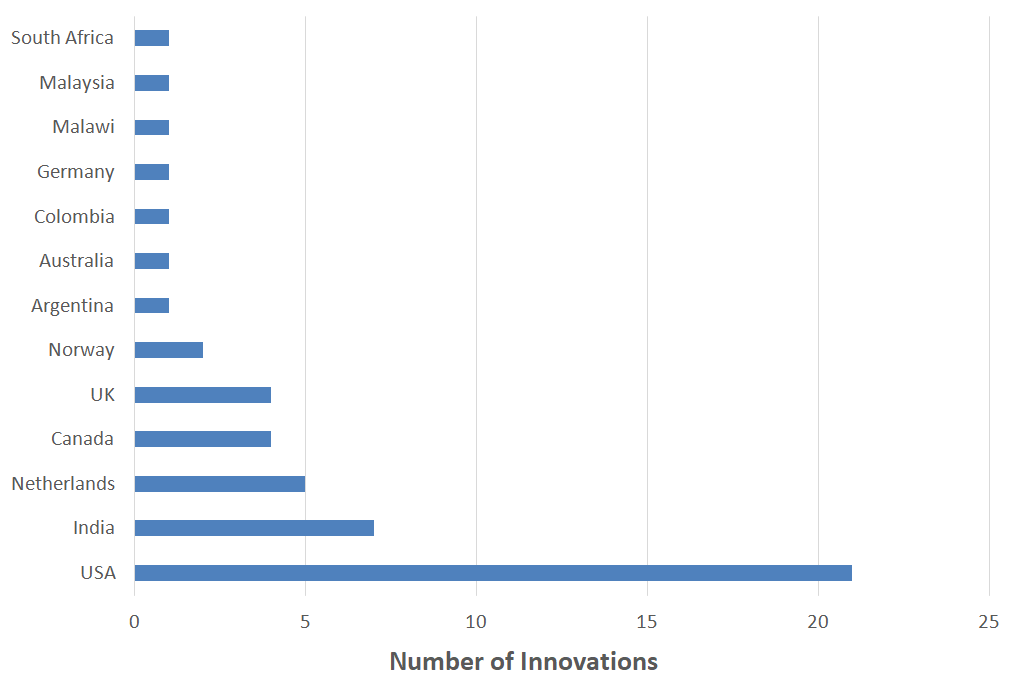
Figure 1. Number of innovations by innovators’ countries of origin
We define the first launch market as the country where the product or service was first launched. Similarly, we segment first launch markets by continent and country classification. As shown in Figure 2, the most popular launch market for healthcare innovations is India, where about a quarter (12 of 50) of the healthcare innovations were first launched. The United States was second with nine launches. As expected, the majority of products were first launched in emerging and developing economies, most of them in Africa (18) and in Asia (15).
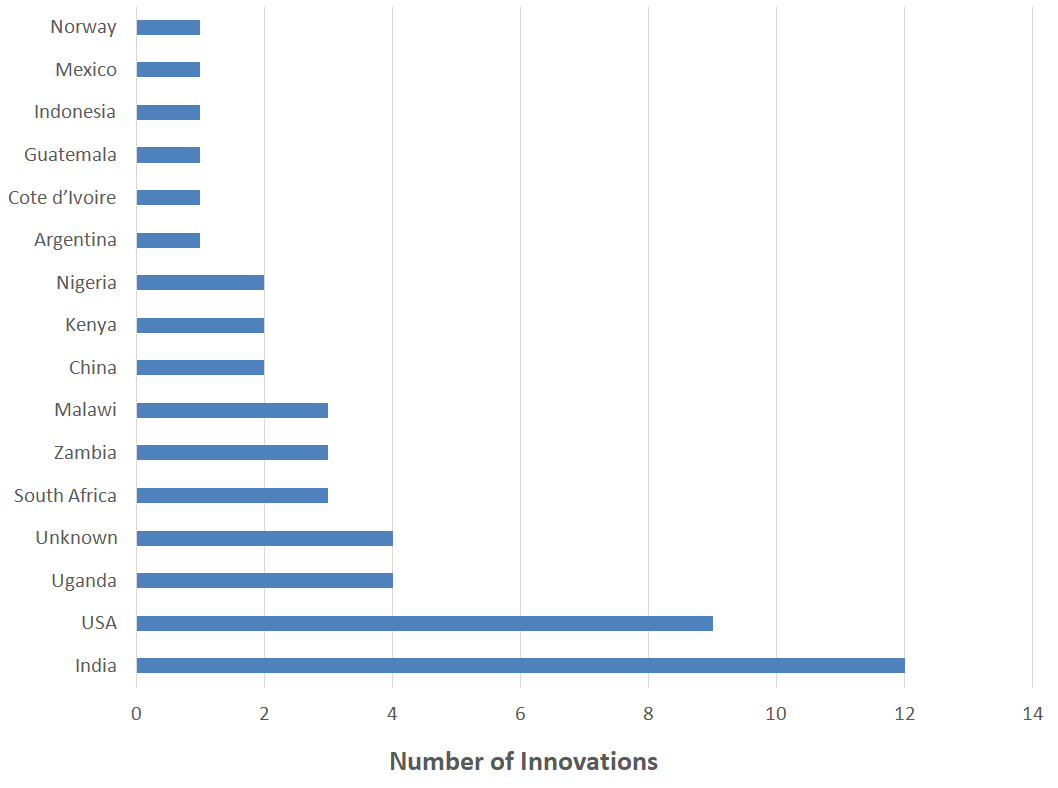
Figure 2. Number of innovations by first launch market
Type of innovator and type of innovation
We differentiated the types of innovators into five different categories: grassroots entrepreneurs, small and medium-sized enterprises (SMEs), multinational companies (MNCs), research/academia, and non-governmental organizations (NGOs). We chose these categories on the one hand to account for the types of innovators that are mentioned in the frugal innovation literature. On the other hand, we chose them to account for the drastically changed innovation process of the 21st century that can be resumed in a shift from a “managed economy” to an “entrepreneurial economy” where small and new firms gain in importance (Audretsch & Thurik, 2004; OECD, 2010; Thurik, 2009). Figure 3 shows that research is the most active innovator type with over 40% of innovations, followed by MNCs and grassroots entrepreneurs with around 25% of innovations respectively. The three groups account for over 90% of all frugal healthcare innovations. NGOs and SMEs play a secondary role in our sample.
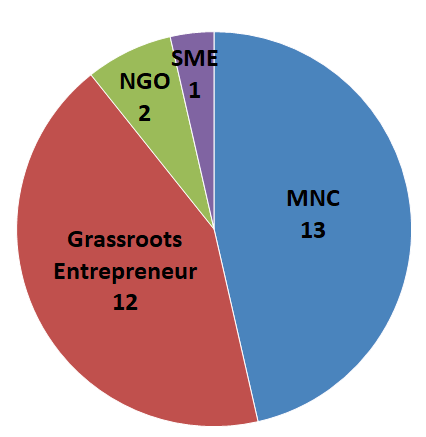
Figure 3. Number of innovations by type of innovator
To determine the types of innovation, we use the classification from the OECD’s Oslo Manual for innovation, which distinguishes between four types of innovations: product, process, marketing, and organizational (OECD, 2005). Figure 4 shows that 76% of the innovations are product innovations. Nine frugal innovations (18%) are process innovations, and three are both product and process innovations (e.g., Kit Yamoyo).We found no marketing and organizational innovations, which is not surprising due to the fact that these tend not to be commercialized.
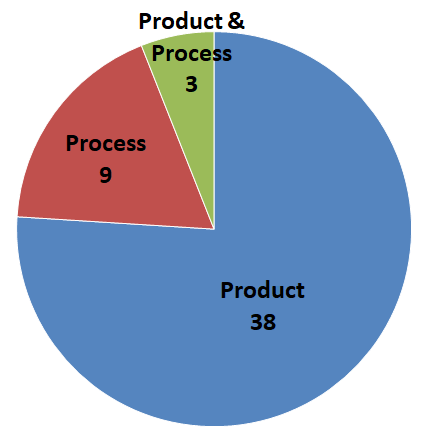
Figure 4. Innovations by type of innovation
Medical specialty and WHO healthcare categories
We also looked into the medical specialty of the frugal innovation (European Parliament and Council, 2005). Overall, the frugal innovations target a wide range of specialties: allergy and immunology, anesthesiology, audiology, cardiology, endocrinology, gastroenterology, general practice, gynecology, medical oncology, neonatology, ophthalmology, orthopedics, otolaryngology, pediatric pulmonology, and radiology (Figure 5). The two most frequent specialties are neonatology and general practice with 11 innovations each, which in part might be driven by funding opportunities from large granting agencies and non-profit organizations. Innovations for general practice include the water purifier Tata Swach, a frugal thermometer (from Leiden University, TU Delft, and Erasmus University), and a portable ventilator (small size, ease of use, and low cost) from Philips. Many innovations are also in the field of orthopedics, including prosthetics such as the Jaipur foot, a rubber-based artificial limb, and Cyborg Beast, a 3D-printed hand prosthetic.
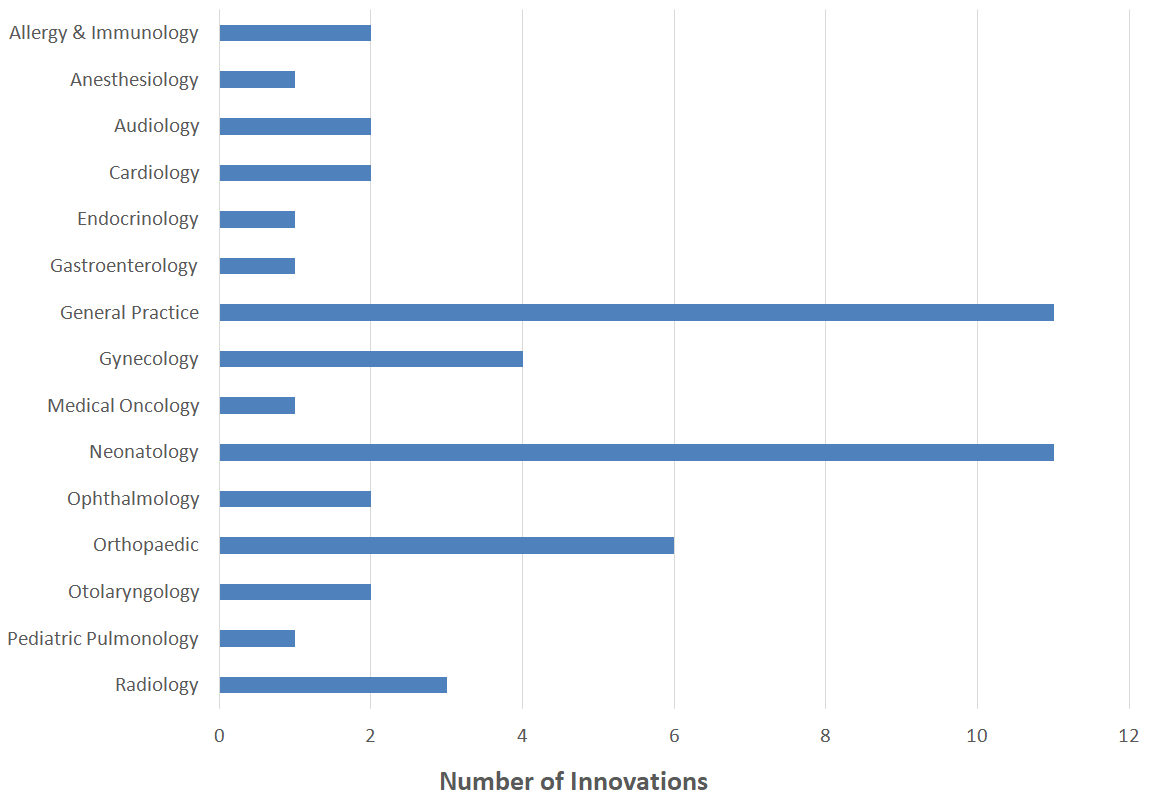
Figure 5. Number of innovations by medical specialty
The WHO tracks progress towards universal health coverage around the world. Universal health coverage means that “all people and communities can use the promotive, preventative, curative, rehabilitative and palliative health services they need” without exposing them to financial hardship (WHO, 2017). We use this classification of health services to analyze which parts of the health continuum are addressed by our sample of frugal innovations (Figure 6). Half of the innovations, and thus the majority, are of preventative character (e.g., Tata Swach). Another third of the frugal innovations are curative (e.g., Kit Yamoyo). Three are rehabilitative (e.g., the Jaipur foot). Six innovations are classified as enablers. A number of frugal innovations, such as bicycle ambulances, allow better access but are not adequately reflected by the categorization, which is why we added a new category and classified them as enablers.
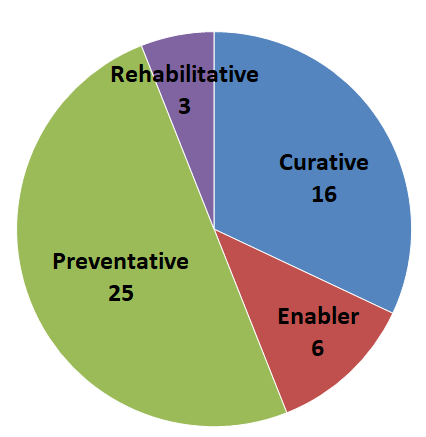
Figure 6. Innovations segmented by WHO healthcare categories
Geographic diffusion
Finally, we tried to assess the success of the innovations in our sample by looking at sales numbers or revenues or number of reached persons. Unfortunately, for most innovations these numbers were not available. We thus chose the geographic diffusion as a proxy. Based on the underlying data, we defined the following spans: i) if the innovation is available in one country only, its geographic diffusion is defined as national ii) multinational diffusion describes an innovation that is available in two to five countries; and, finally, iii) worldwide if it is used or commercialized in more than five countries. Over 40% of innovations have a national focus only (e.g., Kit Yamoyo in Zambia). Almost as many innovations are available in at least five countries, including Embrace, Foldscope, and the Jaipur foot. Eleven innovations have a multinational geographic diffusion.
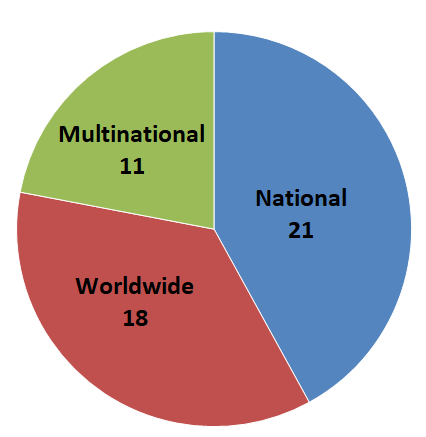
Figure 7. Innovations segmented by geographic diffusion
Type of innovator, entrepreneur’s country of origin, and first launch market
Research innovators in our sample are largely from the United States and Canada (15 and 3 out of 22 innovations respectively). About a third of the group of grassroots entrepreneurs are from India. Europe accounts for almost half of all MNC innovations (6 out of 13 innovations), dominated by the two large European healthcare firms Philips and Siemens. Overall, we find that almost 85% of innovations from MNCs and research are from advanced economies (32 out of 38 innovations) while grassroots entrepreneurs are predominantly from developing countries (7 out of 12 innovations). Research, MNCs, and grassroots entrepreneurs chose developing economies as their first launch market.
Type of innovator and innovation characteristics
Eleven out of 13 MNC innovations in our sample are product innovations; 70% have a preventative focus and 30% a curative focus. Examples are the Tata Swach water purifier or GE Healthcare’s ECG device. From a medical specialty perspective, the innovations mostly fall into the categories of neonatology and general practice, which were the most frequent categories in the total sample.
Research also focuses heavily on developing products (20 out of 22 innovations are product innovations). Compared to MNCs, research focuses on preventative and curative innovations. More than 77% of the 22 research innovations fall into these two categories. In terms of medical specialties, the research innovations can be roughly equally attributed to neonatology, general practice, and orthopedics. Research innovations include the Embrace infant warmer and the Cyborg Beast prosthetic.
Looking at the sample of frugal healthcare innovations that are developed by grassroots entrepreneurs, a different picture emerges. Grassroots entrepreneurs developed almost all process or combined process and product innovations in our sample. In contrast to MNCs and research, they also have a stronger focus on curative innovations, followed by the group of enablers and preventative innovations and cover a wide area of medical specialties.
Type of innovator, characteristics of innovation, and geographic diffusion
Our expectation was that the geographic diffusion of MNC innovations would be higher than for other innovators. Indeed, the descriptive statistics show that almost 60% of grassroots innovations have a national reach only. Another 25% of grassroots entrepreneurs’ innovations are available in a maximum of five countries. In the group of research innovations, 50% have a national focus only. More than 30% of innovations in the group of research innovations are available in more than five countries. Finally, over 50% of MNC innovations are distributed in more than five countries and only 23% are available in one country only.
We also examined how the characteristics of the frugal healthcare innovation correlate with geographic diffusion. In our sample, product innovations have a larger geographic diffusion than process innovations or combined product and process innovations. Out of 12 innovations that are process or combined process and product innovations, only one is available in more than five countries. On the other hand, two thirds of the larger group of product innovations are available in at least two countries, over 40% even in five or more countries.
In terms of WHO healthcare categories, we find that two thirds of all innovations that belong to the group of the so-called enablers are predominantly available in one country only. The picture is more balanced for curative and preventative healthcare innovations. The small group of three rehabilitative innovations all have a reach of five and more countries.
Summary and Conclusion
Despite the relevance of frugal innovations for global health, little research on this topic is available. The objective of this article was to shed more light on this topic and discover patterns of frugal innovations in healthcare. To this aim, we performed a comprehensive literature review and identified 50 frugal healthcare innovations. For these 50 innovations, we retrieved information for different innovation characteristics. We explored the entrepreneur’s country of origin, first launch market, type of innovator, type of innovation, medical specialty, WHO healthcare categories, and geographic diffusion. Our analysis showed some expected and some unexpected results.
The majority of frugal healthcare innovation entrepreneurs in our sample have their origin in the industrialized countries of the world, predominantly in North America and Europe. Overall, the majority of innovations were expectedly first launched in emerging and developing economies compared to advanced economies, most of them in Africa and in Asia. The market where most healthcare innovations are first launched is India, followed by the United States where a lot of research innovations are first launched. Academia is overall the most active innovator in our sample with over 40% of innovations and is dominated by North American stakeholders. These were followed by the group of MNCs, which in our sample contains several companies rooted in Europe and grassroots entrepreneurs with around 25% percent of innovations. Overall, we find that almost 85% percent of innovations from MNCs and research are from advanced economies. They thus play a prominent role in achieving the goals of better health and wellbeing worldwide. Three quarters of the innovations are product innovations. Half of the innovations are of preventative character. Another third of the frugal innovations are curative in their nature. Over 40% of innovations have a limited national diffusion only. Almost as many innovations are available in at least five countries.
MNC innovations in our sample are predominantly product innovators with a preventative focus. From a medical specialty perspective, the innovations mostly fall into the categories of neonatology and general practice, which were also the most frequent categories in the total sample. Combined with the fact that MNCs primarily target preventative innovations, this seems to be an indicator that MNCs take a strategic approach and target the most pressing needs in developing countries. MNC innovations have expectedly the highest geographic diffusion. Over 50% of MNC innovations are distributed in more than five countries and only 23% percent are available in one country only. Product innovations enable scale-up effects and independence from local ecosystem-specific processes.
In terms of medical specialties, research innovations can be roughly equally attributed to neonatology, general practice, and orthopedics. We found that 50% of research innovations have a national focus only, and 30% are available in more than five countries.
Looking at the sample of frugal healthcare innovations that are developed by grassroots entrepreneurs, a different picture emerges. Grassroots entrepreneurs are predominantly from developing countries – especially India, the birthplace of the frugal innovation concept. Grassroots entrepreneurs solve local challenges: they develop almost all process or combined process and product innovations in our sample, which requires in-depth knowledge about processes in local ecosystems. In contrast to MNCs and research, they also have a stronger focus on curative innovations, followed by enablers and preventative innovations and covering a wide area of medical specialties. According to our expectations, the geographic diffusion of grassroots entrepreneurs’ innovations is lower than for MNC and research innovators. Almost 60% of grassroots innovations have a national reach only. Another 25% percent of grassroots entrepreneurs’ innovations are available in a maximum of five countries. All these findings coincide with the view that grassroots entrepreneurs target a specific healthcare need in a country or region and try to develop a frugal product or process without necessarily taking an international perspective. Grassroots entrepreneurs may also not have the infrastructure or business expertise to scale up their solutions.
In order to generate a further impact on global health and wellbeing, the development of frugal innovations should be encouraged by companies, academia, international healthcare organizations, and policy makers in both the advanced and developing parts of the world. MNCs have understood the value of local human resources and their frugal mindsets in developing products for the BOP markets and have gone down this road for several years now. Our analysis shows that grassroots entrepreneurs play a significant complementary role for healthcare systems in developing and emerging countries of the world, because they create solutions for punctual, local, and also processual challenges and are not necessarily driven by strategic scalability and profitability motives. This creativity could be further leveraged through initiatives of governments and international organizations, which bring together different types of innovators and disciplines in order to create knowledge spillovers, bring these ideas to other regions and countries, and support grassroots entrepreneurs to scale up their activities. This could create a positive impact in emerging and developing economies but also bring innovative solutions to industrialized countries that struggle with exploding healthcare costs.
Our study has several limitations. First, the small sample size prevented us from doing formal statistical tests. As stated above, the innovations included in the study may also not be representative of the entire frugal innovation landscape because we only examined articles written in English, meaning it may be biased towards innovations from industrialized countries. Innovations were also excluded if not enough information could be found, which increases the bias against innovations from emerging and developing countries that tend not to have an extensive English website or international partners. Finally, our search terms include only the keywords “frugal innovation” and “healthcare” thereby limiting the search and excluding frugal innovations that are not labelled as such or are labelled under related innovation terms such as jugaad innovation or low-cost innovation. A third limitation is the measurement of success of the innovations in our sample. Due to the unavailability of comparable data on, for example, revenues, profits, treated patients, or sold pieces, we approximated the success of an innovation through the variable geographic diffusion, which is a rather weak indicator. All these limitations provide opportunities for further research. Additional areas for research on frugal innovations lie in the fields of adequate business models or success factors for the diffusion of frugal innovations.
References
Agarwal, N., & Brem, A. 2012. Frugal and Reverse Innovation - Literature Overview and Case Study Insights from a German MNC in India and China. In Proceedings of the 18th International Conference on Engineering, Technology and Innovation (ICE 2012), Munich, Germany, June 18–20, 2012.
https://dx.doi.org/10.1109/ICE.2012.6297683
Allen, L. N., & Christie, G. P. 2016. The Emergence of Personalized Health Technology. Journal of Medical Internet Research, 18(5): e99.
http://doi.org/10.2196/jmir.5357
Anderson, J., & Markides, C. 2007. Strategic Innovation at the Base of the Pyramid. MIT Sloan Management Review, 49(1): 83–88.
Audretsch, D., & Thurik R. 2004. A Model of the Entrepreneurial Economy. International Journal of Entrepreneurship Education, 2(2): 143–166.
Basu, R. R., Banerjee, P. M., & Sweeny, E. G. 2013. Frugal Innovation: Core Competencies to Address Global Sustainability. The Journal of Management for Global Sustainability, 1(2): 63–82.
http://dx.doi.org/10.13185/JM2013.01204
Bhatti, Y., & Ventresca, M. 2013. How Can ‘Frugal Innovation’ Be Conceptualized? Oxford: Said Business School Working Paper Series.
Brem, A., & Wolfram, P. 2014. Research and Development from the Bottom Up – Introduction of Terminologies for New Product Development in Emerging Markets. Journal of Innovation and Entrepreneurship, 3(9): 1–22.
https://doi.org/10.1186/2192-5372-3-9
Clyde, P. 2005. Growing Pains: A Ross School Perspective on the Evolution of the Aravind Eyecare System. Ann Arbor, MI: University of Michigan.
http://www.aravind.org/content/aravindmediapdffiles/journalcasestudies/G...
The Economist. 2010. First Break All the Rules: The Charms of Frugal Innovation. The Economist, April 15, 2010. Accessed April 11, 2018:
https://www.economist.com/node/15879359
European Parliament and Council. 2005. Directive 2005/36/EC of the European Parliament and of the Council of 7 September 2005 on the Recognition of Professional Qualifications. Brussels: European Parliament and Council.
http://data.europa.eu/eli/dir/2005/36/2016-05-24
Hossain, M. 2016. Frugal Innovation: A Systematic Literature Review. Available at SSRN:
http://dx.doi.org/10.2139/ssrn.2768254
IMF. 2017. Country Composition of WEO Groups. International Monetary Fund (IMF), October 2017. Accessed January 7, 2018:
https://www.imf.org/external/pubs/ft/weo/2017/02/weodata/groups.htm (Jan 7, 2018).
Kahle, H. N., Dubiel, A., Ernst, H., & Prabhu, J. 2013. The Democratizing Effects of Frugal Innovation: Implications for Inclusive Growth and State-Building. Journal of Indian Business Research, 5(4): 220–234.
https://doi.org/10.1108/JIBR-01-2013-0008
Khanna, T., Kasturi Rangan, V. & Manocaran, M. 2005. Narayana Hrudayalaya Heart Hospital: Cardiac Care for the Poor. Harvard Business School Case 505-078. Boston, MA: Harvard Business School.
Landrum, N. E. 2007. Advancing the ‘Base of the Pyramid’ Debate. Strategic Management Review, 1(1): 1–12.
OECD. 2005. Oslo Manual: Guidelines for Collecting and Interpreting Innovation Data, (3rd ed.). Paris: Organisation for Economic Cooperation and Development (OECD).
http://dx.doi.org/10.1787/19900414
OECD. 2010. SMEs, Entrepreneurship and Innovation. Paris: Organisation for Economic Cooperation and Development (OECD).
http://dx.doi.org/10.1787/20780990
Oppong, F. C. 2015. Innovation in Income-Poor Environments. British Journal of Surgery, 102(2): 102–107.
https://doi.org/10.1002/bjs.9712
Ostraszewska, Z., & Tylec, A. 2015. Reverse Innovation – How It Works. International Journal of Business & Management, 3(1): 57–74.
https://doi.org/10.20472/BM.2015.3.1.004
Pansera, M., & Sarkar, S. 2016. Crafting Sustainable Development Solutions: Frugal Innovations of Grassroots Entrepreneurs. Sustainability, 8(1): 51.
http://dx.doi.org/10.3390/su8010051
Prahalad, C. K. 2004. The Fortune at the Bottom of the Pyramid: Eradicating Poverty through Profits. Philadelphia: Wharton Business Publishing.
Prahalad, C. K. 2012. Bottom of the Pyramid as a Source of Breakthrough Innovations. Journal of Product Innovation Management, 29(1): 6–12.
https://doi.org/10.1111/j.1540-5885.2011.00874.x
Prahalad, C. K., & Lieberthal, K. 1998. The End of Corporate Imperialism. Harvard Business Review, 76, 68–79.
Prahalad, C. K., & Hart S. L. 2002. The Fortune at the Bottom of the Pyramid. Strategy+Business, 26(1): 55–67.
Prahalad, C. K., & Hammond, A. 2002. Serving the World’s Poor, Profitably. Harvard Business Review, 80(9): 48–57.
PRISMA. 2018. Transparent Reporting Systematic Reviews and Meta-Analyses. PRISMA. Accessed March 23, 2018:
http://prisma-statement.org
Ramdorai, A., & Herstatt C. 2015. Frugal Innovation in Healthcare. How Targeting Low-Income Markets Leads to Disruptive Innovation. Cham, Switzerland: Springer International Publishing.
Rosca, E., Arnold, M., & Bendul, J. C. 2016. Business Models for Sustainable Innovation – An Empirical Analysis of Frugal Products and Services. Journal of Cleaner Production, 162: 133–145.
http://dx.doi.org/10.1016/j.jclepro.2016.02.050
Sarangi, S., Patro, S., & Kumar, R. S. 2014. Sustainable Distribution in Emerging Markets – African Perspective. Transnational Marketing Journal, 2(1): 39–60.
Schumacher, E. F. 1973. Small Is Beautiful – A Study of Economics as If People Mattered. London: Blond and Briggs.
Thurik, R. 2009. Entreprenomics: Entrepreneurship, Economic Growth, and Policy. In Z. Acs, D. Audretsch & R. Strom (Eds.), Entrepreneurship, Growth, and Public Policy: 219–249. Cambridge: Cambridge University Press.
Tiwari, R., Fischer, L., & Kalogerakis, K. 2016. Frugal Innovation in Scholarly and Social Discourse: An Assessment of Trends and Potential Societal Implications. Working Paper. Hamburg and Leipzig, Germany: Center for Frugal Innovation, Hamburg University of Technology, Fraunhofer Center for International Management and Knowledge Economy.
https://doi.org/10.15480/882.1288
Tiwari, R., & Herstatt, C. 2012. Assessing India’s Lead Market Potential for Cost-Effective Innovations. Journal of Indian Business Research, 4(2): 97–115.
https://doi.org/10.1108/17554191211228029
UN. 2015. Sustainable Development Goals: 17 Goals to Transform Our World. United Nations (UN), September 25, 2015. Accessed January 5, 2018:
http://www.un.org/sustainabledevelopment/sustainable-development-goals/
Weyrauch, T., & Herstatt, C. 2016. What Is Frugal Innovation? Three Defining Criteria. Journal of Frugal Innovation, 2(1): 1–17.
https://doi.org/10.1186/s40669-016-0005-y
WHO. 2017. What is Universal Coverage? World Health Organization (WHO). Accessed January 9, 2018:
http://www.who.int/health_financing/universal_coverage_definition/en/
Zeschky, M. B., Winterhalter, S., & Gassmann, O. 2014. From Cost to Frugal and Reverse Innovation: Mapping the Field and Implications for Global Competitiveness. Research-Technology Management, 57(4): 20–27.
https://doi.org/10.5437/08956308X5704235
Keywords: developing economies, emerging economies, frugal innovation, global health, healthcare