AbstractTo know that you do not know is the best.
To think you know when you do not is a disease.
Recognizing this disease as a disease is to be free of it.Lao-Tzu (6th–5th century BC)
Ancient Chinese philosopher
Infection prevention and control has been the subject of much study in medical and epidemiological research and a variety of best practice guidelines have been developed to support healthcare workers and related stakeholders. Yet, despite the availability of information, managing healthcare-associated infections remains a challenge because the relevant explicit knowledge is not being adequately developed and mobilized as tacit knowledge for use "on the front lines". Some researchers have called for a human factors perspective to help address challenges in designing for infection prevention and control, but relatively few studies have been conducted to date. Researchers also suggest that empirical inquiry is needed to better inform the design process, and particularly the design of complex systems where attention to detailed processes and interactions can support the success of an intervention. A human factors approach can help designers develop a deeper understanding of work processes, technology considerations, as well as physiological, psychological, cultural, and organizational factors. The need is particularly pressing in low-resource healthcare environments where funds, time, and human resources may be scarce and strategic design decisions based on evidence are needed to support meaningful and effective changes. With this in mind, a human factors study was conducted in an existing neonatal intensive care unit to identify the influence of product and environment design on infection prevention and control and to inform recommendations for improvement. In this case study, we illustrate how the application of an empirical, methodical approach can help design professionals and stakeholders develop tacit knowledge of complex systems – knowledge that can be used to better inform design priorities, the design process, decision making, and the allocation of resources to help maximize improvements.
Introduction
Every year, more than 200,000 patients in Canada acquire an infection while receiving healthcare and more than 8,000 die as a result (Public Health Agency of Canada, 2013). Infections can arise from the entry and multiplication of a microorganism in a person’s tissue (Public Health Ontario, 2012a, 2012b). As healthcare workers perform tasks, they circulate among patients, objects, and surfaces, thereby creating opportunities for transmitting microorganisms and possibly contributing to the spread of hospital-acquired infections. Newborns hospitalized in neonatal intensive care units are particularly vulnerable because of inherent risk factors such as low birth weight, underlying illness, undeveloped immune systems, and greater skin permeability. Other risk factors include poor staff-to-patient ratios, crowded environments, and exposure to invasive devices (Public Health Ontario, 2012a, 2012b).
These challenges point to the need for more care in the study of design for infection prevention and control. Best practice guidelines and protocols do exist to prevent and control infections; the key challenge is developing and mobilizing the tacit knowledge required to realize the intended improvements.
Currently, there are two basic protocols in infection prevention: i) routine practice, which is a fundamental requirement used on "all patients at all times in all healthcare settings" (Public Health Agency of Canada, 2012) and ii) additional precautions, which include a more rigorous process required when risk assessments performed on a patient suggest extra barriers are needed to mitigate the risk of infection transmission. Four "moments" of hand hygiene (Figure 1) are recommended in routine practice to break the chain of infection transmission. But in neonatal care, five moments are recommended, with an additional hand hygiene step required prior to entering the neonate environment (Public Health Ontario, 2012a). Despite the prevalence of guidelines for infection prevention and control and new technologies focused on improving survival rates and outcomes, infectious complications in neonates is challenging for healthcare institutions (Pessoa-Silva et al., 2007). For example, a survey of 997 pediatric patients across 19 Canadian hospitals revealed that 80 children had a combined total of 91 healthcare acquired infections (or 9.1 % of patients surveyed) (Gravel et al., 2007). The study also showed that the highest prevalence of healthcare associated infections was in the neonate age category. This group was 1.5 times as likely to have a healthcare associated infection than all other groups combined.
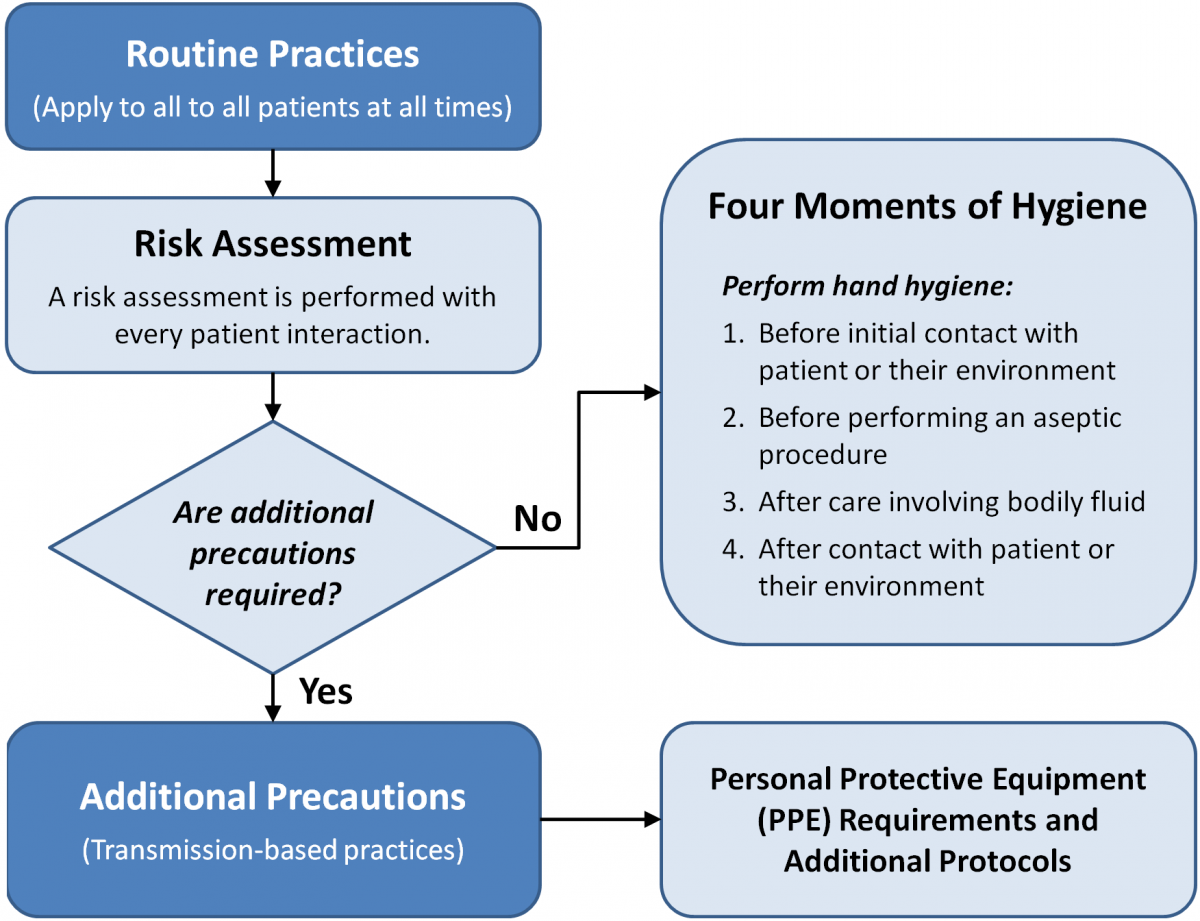
Figure 1. The "four moments" of hand hygiene in routine practice
Some common reasons given for poor compliance with infection prevention measures include: poorly located and insufficient quantities of sinks and hand sanitizers (e.g., Graham, 1990; Muto et al., 2000; Pittet, 2000); poorly located supplies (e.g., Hendrich, 2003); lack of knowledge of protocols or disagreement with protocols (e.g., Pittet, 2001); perceptions that the risk of transmitting infections is low; perceptions that protocols interfere with staff–patient relations; perceptions that patient needs take priority over hand hygiene (e.g., Pittet, 2001); and issues such as understaffing, forgetfulness, insufficient time, and high workload (e.g., Archibald et al., 1997; Pittet, 2001; Ulrich et al., 2004). This brief list illustrates the broad range of considerations in infection prevention and control, and researchers are suggesting that multimodal, multidisciplinary, and systemic approaches are needed to adequately address the scope of issues (Alvarado, 2012; Pessoa-Silva et al., 2007; Pittet, 2001).
Here, we present the results of a study into the challenges of infection prevention and control experienced by a neonatal intensive care unit (NICU) as a case study of the broader issue of knowledge mobilization in complex systems. We discuss the rationale for the study design and briefly outline the methods and the principal outcomes that were developed from applying the approach. The two main outcomes from the study are: i) a framework illustrating what healthcare workers are experiencing in infection prevention and control and how this relates to design and ii) the NICU IPAC [Infection Prevention and Control] Design Exploration Guide, which categorized issues and opportunities for future study and design development.
Another, less obvious outcome that we discuss is the benefits associated with the inquiry process itself in facilitating a deeper knowledge of the issues – knowledge that led to the development of the NICU IPAC Design Exploration Guide. The process required a thorough and systematic approach to data collection and analysis, which we propose helped improve our understanding of the issues healthcare workers are experiencing in infection prevention and control. We provide evidence that suggests human-centred design can deepen our knowledge of complex work and support a more informed path for designing in the field.
The Existing Context and the Need for Pre-Design Investigation
The context of this study, a Level III neonatal intensive care unit (NICU), was renovated prior to the introduction of standards for NICU design, which recommend single patient rooms, appropriate space per infant, and dedicated hand-wash sinks for each patient (White, 2006, 2007). Apart from these basic considerations, stakeholders explained that "adhering to "the five moments" of hand hygiene was difficult due to the nature of their work in relation to the design of products and their environment. As a result, the unit adopted the "four moments" model and zoned the unit into the hospital environment and the patient environment (Figure 2). In this model, healthcare workers were required to perform hand hygiene before contact with each zone, bring only sterile supplies into the patient environment, and disinfect items moving between zones in order to break the potential path of pathogen transmission. Despite reports of high hand hygiene compliance (approximately 90%) during the time of the study, the unit wanted to improve measures to support infection prevention.
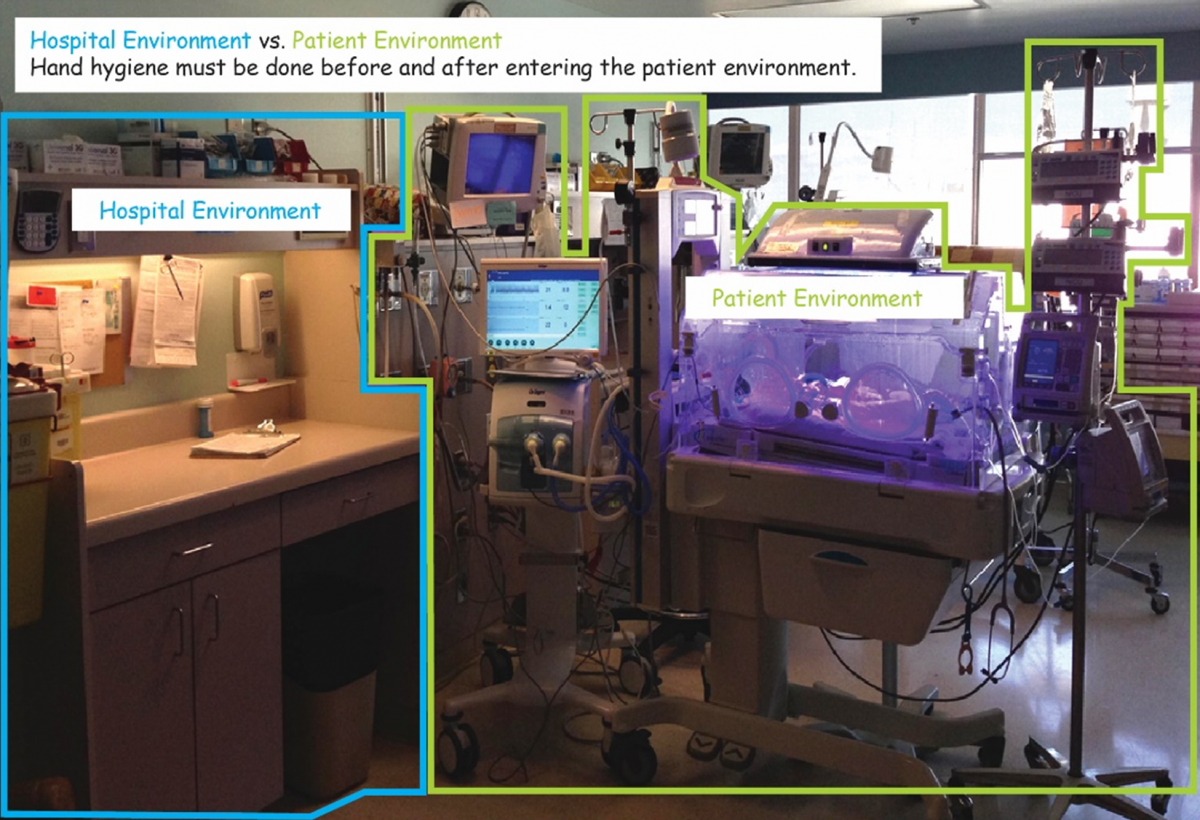
Figure 2. Zoning of the patient environment and the hospital environment in the neonatal intensive care unit
Stakeholders suggested their main challenges in infection prevention and control involved overstocking of bedside supplies, shared equipment, and workflow relationships to products and the environment. The researcher, who had past experience in healthcare design, asked if supply carts had been considered to replace the bedside counter, given that some were capable of being decontaminated, could move with the patient if needed, and might provide opportunities for mounting and organizing supplies and accessories. This suggestion was met with hesitation by stakeholders, who felt this would not resolve their challenges. However, they were interested in studying the issue in greater depth and using the knowledge developed in the study to inform future design initiatives. Considering the health and safety and financial risks involved in developing an effective strategy for improvement, the value of conducting empirical inquiry early on – indeed prior to – developing specific design interventions was clear.
Support for Empirical Inquiry in the Design of Complex Systems
There is growing interest in using empirical inquiry prior to design to help inform development (Brehmer et al., 2014). Friedman (2003) has voiced concerns with designers taking on increasingly complex projects, stating that failures and issues related to design are commonly due to a "lack of method and absence of systematic and comprehensive understanding". In discussing architecture, Remjin (2006) highlights several problems with top-down design approaches, including that they rely too heavily on: the objectives and goals set by management; the past experience of the architect, which may not necessarily fit the project needs; and generalized programmatic requirements, which may not recognize the difficulties and intricacies of complex work. Remjin (2006) notes that, in “a complex work situation it is plausible that practice differs from the expected situation by architect and perception of management” and that this can lead to designs that do not support work processes.
A human factors/ergonomics approach in design focuses on minimizing the effects of constraints, complementing the strengths and abilities of end users, and not forcing people to adapt to undesirable conditions (Chartered Institute of Ergonomics and Human Factors, 2016). These principles are supported by analyzing existing conditions as well as possibilities for new states or situations (Remijn, 2006). The experiences and perspectives of front-line workers, as well as goals set by management, are incorporated to develop a "systems approach" to generating proposals. A systems perspective may also help identify factors that can improve a situation outside the traditional domain of design (e.g., the impact of education and training) or outside a particular field of design (e.g., the impact of product versus architectural design).
The Study Design
Data collection methods from human-centred design frameworks (see ISO 2015,; Maguire, 2001) can help foster a greater understanding of front-line workers, their tasks and objectives, and the greater work context (Rogers et al., 2012). Data collection methods for human-centred design, such as naturalistic observation, encourage participant feedback during observations, which can help people — particularly in complex work — explain what they do (Rogers et al., 2012).
With regards to analyzing data, thematic analysis respects the natural context of the phenomenon by integrating the views and experiences of participants to support an in-depth understanding of their situation (Vaismoradi et al., 2013). The process involves familiarizing oneself with the data, generating codes, searching for themes among codes, and defining themes to produce a framework (Braun & Clarke, 2006) that can move analysis beyond describing individual experiences (Guest et al., 2012) to theorizing why certain behaviours are prevalent. Coding actions keeps the codes tied to activities, reducing the tendency "to make conceptual leaps” from the data (Charmaz, 2014) and helps support the validity of the interpretation (Saldaña, 2009). The resulting framework serves as an organizing principle for illustrating and disclosing the interpretation of the data to the researcher and translating knowledge to a wider audience (Attride-Stirling, 2001).
These methods were selected to identify breaches in infection prevention, behavioural patterns and perceptions related to observed breaches, and the potential influence of design on infection prevention practice. The methods were chosen to help generate a framework that illustrates the issues staff are experiencing, to verify this understanding with stakeholders, and to guide recommendations for future study or design development.
Approach
The study took place in a Level III NICU primarily at the patient bedside, where the majority of patient contact occurs. Field notes, photos, and sketches were used to document the site, comments from stakeholder meetings, observations, and participation of 81 healthcare workers (e.g., nurses, respiratory therapists, housekeepers, supply workers, physicians, technicians). Fifty hours of observations in 4-hour intervals were conducted over the course of twelve shifts on weekdays and weekends, distributed equally over a 24-hour work cycle, covering the beginning, middle, and end of shifts. Observing a large pool of healthcare workers for 50 hours during a 24-hour work cycle produced a rich dataset.
Thematic analysis took place throughout the collection of information. The researcher assigned action codes to the data and wrote memos that captured reflections throughout the study about what was being observed but also on the study process itself. The process helped "chunk" (or categorize) the data into themes, which led to a final framework outlining the main issues healthcare workers are experiencing in infection prevention and control and a recommendations guide to assist the unit with future developments.
Findings
The study revealed that healthcare workers lack a shared mental model of infection prevention and that design is failing to support a shared, functional model. In some cases, the model was functional, with some healthcare workers taking extra precautions in infection-prevention practice beyond what would be required. Other healthcare workers exhibited hazy or faulty models, which resulted in lapses or breaches in infection-prevention practice. The study also showed that the design failed to provide appropriate or clear cues, space requirements, and other necessary attributes to support the understanding and practice of infection prevention and control. This core theme was illustrated in a larger framework of understanding and helped in the development of a recommendations guide to support future initiatives for improvement. For more detailed information on the overall study findings and framework, please refer to Trudel and colleagues (2016a, 2016b). Apart from these findings, with a particular focus on knowledge mobilization and study design, we asked:
- What evidence is there to suggest that the methods themselves fostered a deeper understanding of the experience of healthcare workers in infection-prevention practice?
- Can this approach help inform and strengthen strategies for design development?
Evidence for the value of the approach
The use of multiple data-collection methods and media led to a rich dataset of the environment, products, equipment, supplies, work processes, participant behaviour, and participant comments. Spending 50 hours on the unit over a 24-hour work cycle allowed the researcher to observe processes related to infection prevention and control that occur only at specific points in the work cycle (e.g., blood work, rounds). The data and insights from observing such processes may be missed in design approaches that rely predominantly on collecting information from user-group meetings held outside the unit or during regular work hours. Participant comments and observations demonstrate that the methods helped clarify misinterpretations or correct assumptions held by the researcher (Box 1). Observing front-line staff on site helped them discuss the complexities of their work and infection prevention and control in relation to the existing design, allowing them to physically illustrate the issues and suggest possibilities for improvement.
|
Box 1. Examples of observation scenarios and participant quotations The scenarios below illustrate the rich detail that came from the participation of healthcare workers in the study and how methods from human-centred design such as naturalistic observation and stakeholder meetings can help clarify unknowns or misinterpretations about the context within which infection prevention and control is practiced. Scenario 1: Routine Checks Researcher (speaking to Nurse A): “Can you explain what you’re doing when you silence the alarms?” Nurse A: “The oxygen saturation levels usually drop when an infant comes close to the end of a feeding since the stomach expands and compresses the diaphragm and lungs. When this happens the physiological monitor alarm rings off warning that oxygen saturation levels are low. The nurses then adjust the siPAP or biPAP to adjust the oxygen supply to increase oxygen saturation. With the IV pumps, the alarm might go after telling me the infusion is complete or the rate we’ve set it at is complete.” Researcher: (watching Nurse B set up feeding supplies in the corner of the work surface closest to the bedside): “Why do you set them up there?” Nurse B: “To avoid going in the drawers.” Researcher (speaking to Nurse B): “Why have you left the stethoscope on the cot instead of putting it back on the blender?” Nurse B: “I’ll be using it again and it reminds me to disinfect it before putting it back.” Scenario 2: Feeding Researcher: I move to room 2 to observe. Nurse D is feeding the infant in one of the parent chairs. Nurse E is burping the infant within the isolette, her arms and body are in an awkward posture. I missed where Nurse E’s infant was fed. Nurse D and Nurse E are each taking care of two infants. After burping the infant, Nurse E is trying to set up a feeding syringe to give the remainder of the feed by gravity in the incubator. Researcher (speaking to Nurse E): “Can you explain what you’re setting up?” Nurse E: “When infants are not at risk for regurgitating and are capable of handling a gravity feed we will set up this way. But if the feed amount is really large we will put it in the syringe pump and set the flow rate to suit the infant’s status.” Researcher: Nurse E struggles a bit with setting up the gravity feed trying to use the ventilator tubing holder but this is not working well: it keeps dropping out. Nurse E: “The tube is too rigid and the holder’s not the right size.” Scenario 3: The Family Chair Researcher (speaking to Nurse F): “I’m confused about the family chair because from my understanding it’s part of the hospital environment yet it’s just dawned on me that infants are pulled out and fed in these chairs. Are the chairs disinfected between use, what about the arms in particular or the top of the chair?” Nurse F: (looking a little crestfallen by my question): “But they need to be held.” (understandably a bit defensive). Researcher: “I understand and know how important it is to hold the infant, but I’m trying to understand the chair in relation to infection prevention.” The conversation is informal. No one else is in the room and I am sitting beside her in one the family chairs as she sits in another. Nurse F looks up in the air, pausing (to reflect?) as she continues to feed the infant. Nurse F: “I never thought about it, but yes feeding in the chair, that could be a problem. I touch the arm, I stroke the infant’s head: that’s a breach. I’ve always thought about it as the seat being the issue but I never thought about the arms. We had a mum once who was a carrier of MRSA [infection]. Even though she doesn’t have it, she can spread it to the infants. The mum would be sitting in the chair, she’d get up and I’d wipe it down every time she used it. But I never really thought about the chair otherwise. I would question the chair... my hands are going to go to that arm and then go to another chair. I try to kick things out of the way, but it makes so much noise... I try to do a lot with my feet.” |
Field notes and codes were reviewed during and after the observation to produce a thematic framework illustrating the relationship between design and infection prevention and control. This process helped the researcher "chunk" codes into categories (Table 1), identify dominant categories, identify relationships between categories, and develop a high-level, systemic picture of the experience with infection prevention and control within the unit. Recurring words from the dataset were also assessed. Whereas the frequency of some words could perhaps be foreseen (e.g., isolette, supplies, bedside counter), others were not readily anticipated by the researcher (e.g., drawers, chart, walking), suggesting more detailed investigation may be needed in these areas.
Table 1. Examples of early themes from process coding
|
Example Themes |
Process Codes |
|
Handling the baby with physical barriers
|
|
|
Chart intricately tied to caring for the baby |
|
|
Trying to carve out a “safe space”
|
|
The researcher’s memos (Table 2) demonstrate that using empirical and systematic methods prior to design may help deepen our understanding of the experience of healthcare workers in infection prevention and control and may inform recommendations for further research and design development. The memos illustrate:
- missing details or micro-interactions relevant to infection prevention and control, which required verification in subsequent observations
- considerations in infection prevention and control that needed clarification by participants to deepen the understanding of processes and constraints
- aspects of the context that were striking, not previously known, or not understood
- sensitivities around infection prevention and control and discussing it with participants
- benefits of the method and strategies to improve the method
- thoughts on future research and design development
Table 2. Examples of researcher memos
|
Topic |
Example Memos |
|
Identifying lapses in observation - missed interactions relevant to IPAC |
|
|
Identifying lack of clarity in what constitutes a breach or best practice in IPAC |
|
|
Awareness and questions emerging from observations |
|
|
Thoughts on sensitivities around IPAC |
|
|
Thoughts on method |
|
|
Thoughts on future explorations to investigate, test, evaluate design requirements |
|
Discussion
Early empirical and systematic inquiry and accountability in design
As noted earlier, the researcher had initially suggested perhaps replacing the existing work counter with a supply cart to help with issues around infection practice, a suggestion which was met with some hesitation by stakeholders. At the time, this exchange did not seem significant, but it gained importance during the study. Applying a qualitative, multi-method approach focused primarily on the experiences and perceptions of front-line workers led to a better understanding of this hesitation and the complex challenges healthcare workers had been contending with in infection prevention and control.
It is not clear whether a traditional "top-down" design approach as described by Remijn (2006) would have yielded the same depth in data collected or the level of analysis and recommendations that resulted from the approach. The changes that occurred in the researcher’s own level of understanding of the healthcare workers' experiences of infection prevention and control, evidenced by field notes, memos, and the process of thematic analysis, suggest that early empirical and systematic inquiry can help support design development and perhaps improve accountability in design.
Challenges and opportunities in the method
The main advantage of conducting empirical inquiry prior to design is to help deepen our understanding of end users and their workspace in order to inform design requirements for subsequent development. Developing a framework that structures the main issues end users are experiencing in their workplace can help designers assess whether their understanding of the issues is comprehensive and resonates with that of stakeholders. The results of this study, the framework and the NICU IPAC [Infection Prevention and Control] Design Exploration and have been shared with the leadership team and the organization is working towards a major renovation of the unit to address these challenges. Requirements may change as the design progresses and new information is discovered. A framework that outlines the main issues healthcare workers are experiencing and a design guideline, can help assess the introduction of new information and refinement of requirements.
Additional measures could have increased the depth of the analysis. More detailed and comprehensive data related to specific work domains and data from unavailable stakeholders may have helped fill gaps in "the work system approach" to understanding infection prevention (Alvarado, 2013). Other challenges included the fast pace of work and vigilant observation of micro-interactions that may be associated with breaches in infection prevention and control. But transcribing and process coding field notes after an observation session helped reveal micro-interactions or steps in work processes that had been missed. Memos were also helpful in catching such lapses and informing subsequent observation strategies.
The use of naturalistic observation may be criticized for encouraging "appropriate" behaviour. But, because the approach was non-punitive, the identity of front-line workers was protected, and the study emphasized the importance of front-line participation, this may have in fact helped support natural behaviour. The study time frame limited the extent and type of methods that could be implemented, but future work would ideally include:
- participatory development and assessment of mockups to draw out more information and insight on infection prevention issues and possibilities for improvement
- post-occupancy evaluation of design proposals in simulations or lower acuity areas supported by statistical analysis
Is the method sustainable?
Implementing this type of approach may be met with resistance, because it goes beyond a traditional design scope. At the same time, the term "evidenced-based design", which involves basing designs “on credible research to achieve the best possible outcomes” (The Centre for Health Design, 2016) is becoming increasingly required in healthcare design. Organizations should be able to demonstrate that they have resources and strategies in place to truly support a design process that is based in evidence. The use of systematic, empirical, and multi-method approaches can help support evidence-based practice and accountability over processes that depend solely on the past experience of designers, goals set by management, or generalized programs (Remjin, 2003), or approaches that rely predominantly on unsystematic or singular techniques to understand the issues.
Some may argue this level of inquiry compromises "the bottom line". However, discovering critical issues early can inform design requirements, improve the focus and consensus-building ability of the client-design team, and provide a better measure for evaluation. Further, without implementing such a strategy, how can an organization truly know if it will negatively impact the bottom line without the evidence to support this assumption? Organizations may also consider partnering with academic institutions to pilot and measure such initiatives to mitigate against the risks of developing and integrating "research systems" into an organization’s culture and strategic plan.
Conclusion
This study demonstrates how early empirical and systematic inquiry using methods from human-centred design and thematic analysis led to a framework of understanding and a recommendations guide to help stakeholders improve their understanding and practice of infection prevention. Specifically, the study provides evidence illustrating how our own understanding of designing for healthcare was clarified, broadened, and changed through the application of scientific methods in design. In applying such approaches, we can help professional designers gain the necessary knowledge to make better decisions in the design of complex systems, and at a broader level, sensitize a new generation of designers to the importance of rigour in knowledge acquisition, transfer, application, and assessment.
References
Alvarado, C. J. 2012. Human Factors and Ergonomics in Infection Prevention. In P. Carayon (Ed.), Handbook of Human Factors and Ergonomics in Healthcare and Patient Safety (2nd Ed.): 793–802. Boca Raton, FL: CRC Press.
Archibald, L. K., Manning, M. L., Bell, L. M., Banerjee, S., & Jarvis, W. R. 1997. Patient Density, Nurse-To-Patient Ratio and Nosocomial Infection Risk in a Pediatric Cardiac Intensive Care Unit. The Pediatric Infectious Disease Journal, 16(11): 1045–1048.
http://dx.doi.org/10.1097/00006454-199711000-00008
Attride-Stirling, J. 2001. Thematic Networks: An Analytic Tool for Qualitative Research. Qualitative Research, 1(3): 385–405.
http://dx.doi.org/10.1177/146879410100100307
Braun, V., & Clarke, V. 2006. Using Thematic Analysis in Psychology. Qualitative Research in Psychology, 3(2): 77–101.
http://dx.doi.org/10.1191/1478088706qp063oa
Brehmer, M., Carpendale, S., Lee, B., & Tory, M. 2014. Pre-Design Empiricism for Information Visualization: Scenarios, Methods, and Challenges. In H. Lam, P. Isenberg, T. Isenberg, & F. M. Sedlmair (Eds.), Proceedings of the ACM Workshop on beyond Time and Errors: Novel Evaluation Methods for Visualization (BELIV): 147–151. New York: ACM.
http://dx.doi.org/10.1145/2669557.2669564
The Centre for Health Design. 2016. EDAC: Evidence-Based Design Accreditation and Certification. The Centre for Health Design. Accessed June 4th, 2016:
https://www.healthdesign.org/certification-outreach/edac/about
Charmaz, K. 2014. Constructing Grounded Theory (2nd ed.). London, England: Sage Publications Ltd.
Chartered Institute of Ergonomics and Human Factors. 2016. What Is Ergonomics? Chartered Institute of Ergonomics and Human Factors. Accessed August 9th, 2016:
http://www.ergonomics.org.uk/what-is-ergonomics/
Friedman, K. 2003. Theory Construction in Design Research: Criteria: Approaches, and Methods. Design Studies, 24(6): 507–522.
http://dx.doi.org/10.1016/S0142-694X(03)00039-5
Graham, M. 1990. Frequency and Duration of Handwashing in an Intensive Care Unit. American Journal of Infection Control, 18(2): 77–81.
http://dx.doi.org/10.1016/0196-6553(90)90085-7
Gravel, D., Matlow, A., Ofner-Agostini, M., Loeb, M., Johnston, L., Bryce, E., Sample, M-L., Roth, V. R., Goldman, C., Taylor, G., & The Canadian Nosocomial Infection Surveillance Program. 2007. A Point Prevalence Survey of Health Care–Associated Infections in Pediatric Populations in Major Canadian Acute Care Hospitals. American Journal of Infection Control, 35(3): 157–162.
http://dx.doi.org/10.1016/j.ajic.2006.06.006
Guest, G., MacQueen, K. M., & Namey, E. E. 2012. Applied Thematic Analysis. Los Angeles, CA: Sage Publications.
Hendrich, A. 2003. Optimizing Physical Space for Improved Outcomes: Satisfaction and the Bottom Line. Optimizing the Physical Space for Improved Outcomes, Satisfaction, and the Bottom Line. Mini-Course Sponsored by the Institute for Healthcare Improvement and the Center for Health Design, Atlanta, GA.
ISO. 2015. ISO 9241-210:2010 Ergonomics of Human-System Interaction. Part 210: Human-Centred Design for Interactive Systems. International Organization for Standardization (ISO). Switzerland: ISO Copyright Office. Accessed August 11th, 2016:
http://www.iso.org/Iso/Home/Store/catalogue_ics/catalogue_detail_ics.Htm...
Maguire, M. 2001. Methods to Support Human-Centred Design. International Journal of Human-Computer Studies, 55(4): 587–634.
http://dx.doi.org/10.1006/Ijhc.2001.0503
Muto, C. A., Sistrom, M. G., & Farr, B. M. 2000. Hand Hygiene Rates Unaffected by Installation of Dispensers of a Rapidly Acting Hand Antiseptic. American Journal of Infection Control, 28(3): 273–276.
http://dx.doi.org/10.1067/Mic.2000.103242
Public Health Agency of Canada. 2012. Routine Practices and Additional Precautions for Preventing the Transmission of Infection in Healthcare Settings. Ottawa: Public Health Agency of Canada. http://publications.gc.ca/collections//collection_2013/aspc-phac/HP40-83...
Public Health Agency of Canada. 2013. The Chief Public Health Officer's Report on the State of Public Health in Canada, 2013: Infectious Disease – The Never-Ending Threat. Ottawa: Public Health Agency of Canada.
http://www.phac-aspc.gc.ca/cphorsphc-respcacsp/2013/infections-eng.php
Public Health Ontario. 2012a. Best Practices for Infection Prevention and Control in Perinatology: In All Health Care Settings That Provide Obstetrical and Newborn Care. Toronto: Public Health Ontario, Provincial Infectious Diseases Advisory Committee (PIDAC).
https://www.publichealthontario.ca/en/erepository/IPC%20in%20Perinatolog...
Public Health Ontario. 2012b. Best Practices for Infection Prevention and Control Programs in Ontario: In All Health Care Settings (3rd ed). Toronto: Public Health Ontario, Provincial Infectious Diseases Advisory Committee (PIDAC).
http://www.publichealthontario.ca/en/eRepository/BP_IPAC_Ontario_HCSetti...
Pessoa-Silva, C. L., Hugonnet, S., Pfister, R., Touveneau, S. Dharan, S., Posfay-Barbe, K., & Pittet, D. 2007. Reduction of Health Care-Associated Infection Risk in Neonates by Successful Hand Hygiene Promotion. Pediatrics, 120(2): e382–e390.
http://dx.doi.org/10.1542/Peds.2006-3712
Pittet, D. 2000. Improving Compliance with Hand Hygiene in Hospitals. Infection Control Hospital Epidemiology, 21(6): 381–386.
http://dx.doi.org/10.1086/501777
Pittet, D. 2001. Improving Adherence to Hand Hygiene Practice: A Multidisciplinary Approach. Emerging Infectious Diseases, 7(2): 234–240.
http://dx.doi.org/10.3201/eid0702.700234
Remijn, S. L. M. 2006. Integrating Ergonomics into the Architectural Design Processes: Tools for User Participation in Hospital Design. In Proceedings of IEA 2006 16th World Congress on Ergonomics: Meeting Diversity in Ergonomics, Maastricht, Netherlands: 10–14.
Rogers, Y., Sharp, H., & Preece, J. 2012. Interaction Design – Beyond Human Computer Interaction (3rd ed.). West Sussex, England: John Wiley & Sons Ltd.
Saldaña, J. 2009. The Coding Manual for Qualitative Researchers. Los Angeles, CA: Sage Publications.
Trudel, C., Cobb, S., Momtahan, K., Brintnell, J., & Mitchell, A. 2016a. A Human Factors Approach to Understanding and Designing for Infection Prevention and Control in a Neonatal Intensive Care Unit. Paper presented at Ergonomics & Human Factors 2016, Daventry, United Kingdom, Chartered Institute of Ergonomics & Human Factors.
http://programme.exordo.com/ehf2016/Delegates/Presentation/48/
Trudel, C., Cobb, S., Momtahan, K., Brintnell, J., & Mitchell, A. 2016b. Disconnects in Design and Infection Prevention and Control – How the Design of Products and the Environment in Neonatal Intensive Care May Be Undermining Infection Prevention Practice. Proceedings of the International Symposium on Human Factors and Ergonomics in Health Care June 2016, 5(1): 44–49.
Ulrich, R., Quan, X., Zimring, C., Joseph, A., & Choudhary, R. 2004. The Role of the Physical Environment in the Hospital of the 21st Century: A Once-In-A-Lifetime Opportunity. Concord, CA: The Center for Health Design.
Vaismoradi, M., Turunen H., & Bondas, T. 2013. Content Analysis and Thematic Analysis: Implications for Conducting a Qualitative Descriptive Study. Nursing & Health Sciences, 15(3): 398–405.
http://dx.doi.org/10.1111/nhs.12048
White, R. D. 2006. Recommended Standards for the Newborn ICU. Journal of Perinatology, 26: S2–S18.
http://dx.doi.org/10.1038/sj.jp.7211587
White, R. D. 2007. Recommended Standards for the Newborn ICU. Journal of Perinatology, 27(Suppl 2): S4–S19.
http://dx.doi.org/10.1038/sj.jp.7211837
Keywords: design research, ergonomics, healthcare design, human factors, infection prevention and control, knowledge mobilization, neonatal intensive care unit